Fill Out Your New Mexico Report Form
The New Mexico Employers' First Report of Injury or Illness form is a vital document within the state's workers' compensation framework, designed to detail incidents of injury or illness that occur in the workplace. Required by the New Mexico Workers' Compensation Administration, this form serves multiple purposes: it notifies the agency of work-related injuries or illnesses that result in more than seven days of lost work or result in death, and it acts as a record for both employers and the state to monitor workplace safety and enforce regulations. It is essential for employers to fill out this form accurately and promptly, within 10 days of knowledge of the injury or illness, even if there is a dispute regarding the work-related nature of the injury or illness. The form encompasses several critical pieces of information, including employer and carrier details, the incident specifics—such as the type of injury or illness, how the injury or illness occurred, the date and time of the event, and details regarding the affected employee. Importantly, completing this form does not admit liability under the Workers' Compensation Act. It also outlines penalties for non-compliance, reinforces the need for legible and complete submissions, and provides the employer with the option to continue the injured or ill employee's salary without utilizing their benefits. It underscores the rights and responsibilities of workers and employers while offering guidance on how to report incidents effectively, aiming to ensure the well-being of employees and maintain a safe working environment.
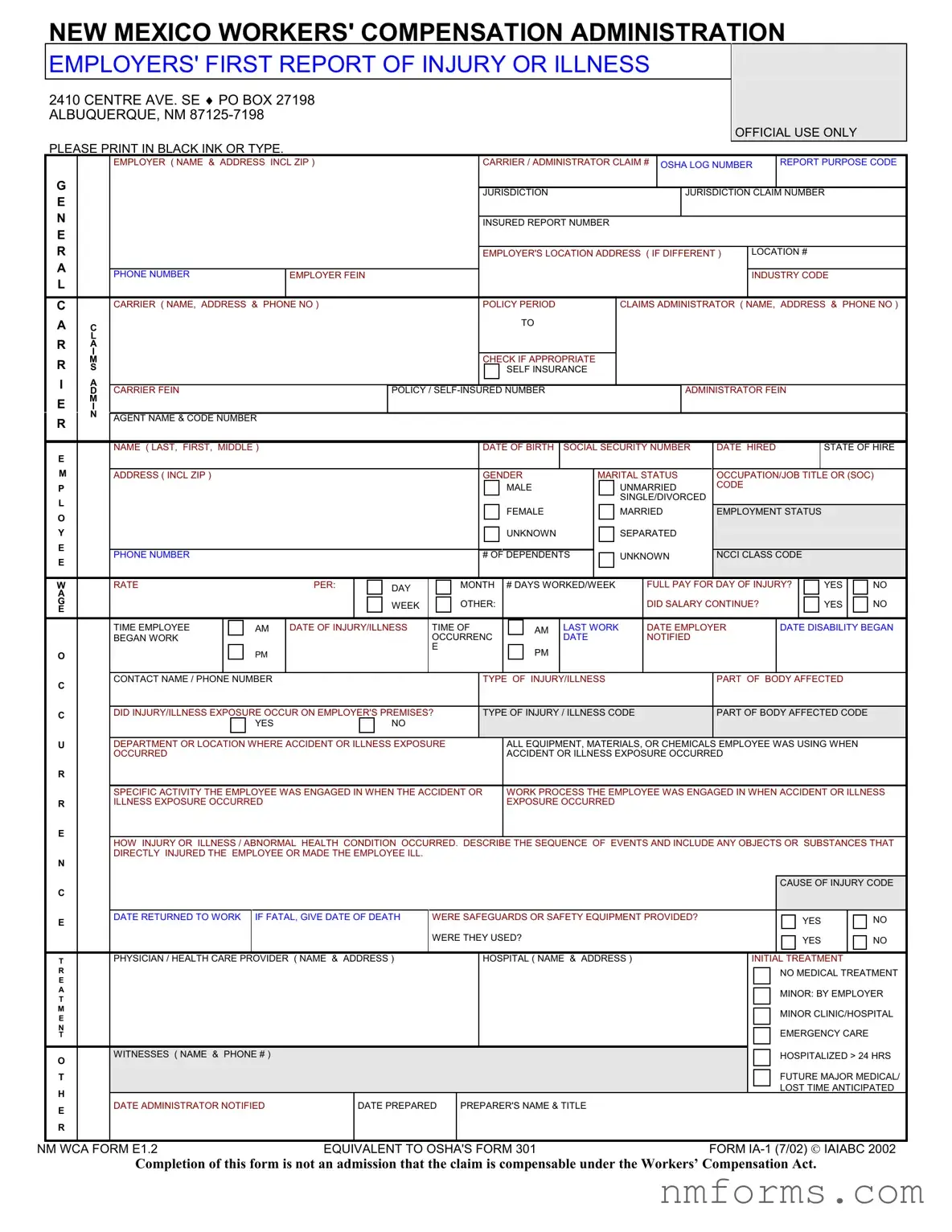
New Mexico Report Sample
NEW MEXICO WORKERS' COMPENSATION ADMINISTRATION
EMPLOYERS' FIRST REPORT OF INJURY OR ILLNESS
2410 CENTRE AVE. SE ♦ PO BOX 27198 ALBUQUERQUE, NM
OFFICIAL USE ONLY
PLEASE PRINT IN BLACK INK OR TYPE.
EMPLOYER ( NAME & ADDRESS INCL ZIP ) |
CARRIER / ADMINISTRATOR CLAIM # OSHA LOG NUMBER |
REPORT PURPOSE CODE |
G |
|
|
|
|
|
|
|
|
E |
|
|
|
|
JURISDICTION |
|
JURISDICTION CLAIM NUMBER |
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
INSURED REPORT NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
||
|
|
|
|
EMPLOYER'S LOCATION ADDRESS ( IF DIFFERENT ) |
LOCATION # |
|||
A |
|
|
|
|
|
|
|
|
|
PHONE NUMBER |
EMPLOYER FEIN |
|
|
|
|
INDUSTRY CODE |
|
L |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
CARRIER ( NAME, ADDRESS & PHONE NO ) |
|
POLICY PERIOD |
CLAIMS ADMINISTRATOR ( NAME, ADDRESS & PHONE NO ) |
|||
A |
C |
|
|
TO |
|
|
|
|
|
|
|
|
|
|
|||
|
L |
|
|
|
|
|
|
|
RA I
R |
M |
|
|
|
|
|
|
|
CHECK IF APPROPRIATE |
|
|
|
|
|
|
|
|
|
|
|
|||||
S |
|
|
|
|
|
|
|
|
SELF INSURANCE |
|
|
|
|
|
|
|
|
|
|
|
|||||
I |
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
CARRIER FEIN |
|
|
|
POLICY / |
|
|
|
|
ADMINISTRATOR FEIN |
|
|
|
|
||||||||||
E |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
N |
AGENT NAME & CODE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
NAME ( LAST, FIRST, MIDDLE ) |
|
|
|
|
|
DATE OF BIRTH |
SOCIAL SECURITY NUMBER |
DATE HIRED |
|
|
|
STATE OF HIRE |
|||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
ADDRESS ( INCL ZIP ) |
|
|
|
|
|
|
GENDER |
|
MARITAL STATUS |
OCCUPATION/JOB TITLE OR (SOC) |
||||||||||||||
P |
|
|
|
|
|
|
|
|
|
MALE |
|
|
UNMARRIED |
CODE |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SINGLE/DIVORCED |
|
|
|
|
|
|
|
|
||
O |
|
|
|
|
|
|
|
|
|
FEMALE |
|
|
MARRIED |
EMPLOYMENT STATUS |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
|
|
|
|
|
|
|
|
|
UNKNOWN |
|
|
SEPARATED |
|
|
|
|
|
|
|
|
||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
PHONE NUMBER |
|
|
|
|
|
|
# OF DEPENDENTS |
|
UNKNOWN |
NCCI CLASS CODE |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
|
RATE |
|
PER: |
|
DAY |
|
MONTH |
# DAYS WORKED/WEEK |
|
FULL PAY FOR DAY OF INJURY? |
|
YES |
|
NO |
||||||||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G |
|
|
|
|
|
WEEK |
|
OTHER: |
|
|
|
|
|
|
DID SALARY CONTINUE? |
|
|
|
YES |
|
NO |
||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
TIME EMPLOYEE |
AM |
DATE OF INJURY/ILLNESS |
TIME OF |
|
|
AM |
LAST WORK |
|
DATE EMPLOYER |
DATE DISABILITY BEGAN |
|||||||||||||
|
|
BEGAN WORK |
|
|
|
|
OCCURRENC |
|
|
|
DATE |
|
NOTIFIED |
|
|
|
|
|
|
|
|
||||
|
|
|
PM |
|
|
|
E |
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
C |
|
CONTACT NAME / PHONE NUMBER |
|
|
|
|
|
TYPE OF INJURY/ILLNESS |
|
|
|
PART OF BODY AFFECTED |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
C |
|
DID INJURY/ILLNESS EXPOSURE OCCUR ON EMPLOYER'S PREMISES? |
|
TYPE OF INJURY / ILLNESS CODE |
PART OF BODY AFFECTED CODE |
|
|
||||||||||||||||||
|
|
YES |
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U |
|
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE |
|
|
ALL EQUIPMENT, MATERIALS, OR CHEMICALS EMPLOYEE WAS USING WHEN |
|
|
||||||||||||||||||
|
|
OCCURRED |
|
|
|
|
|
|
|
ACCIDENT OR ILLNESS EXPOSURE OCCURRED |
|
|
|
|
|
|
|
||||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR |
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS |
||||||||||||||||||||||
R |
|
ILLNESS EXPOSURE OCCURRED |
|
|
|
|
|
|
EXPOSURE OCCURRED |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E
HOW INJURY OR ILLNESS / ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL.
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CAUSE OF INJURY CODE |
|
||
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
DATE RETURNED TO WORK |
IF FATAL, GIVE DATE OF DEATH |
WERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED? |
|
|
YES |
|
NO |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
WERE THEY USED? |
|
|
YES |
|
NO |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
PHYSICIAN / HEALTH CARE PROVIDER ( NAME & ADDRESS ) |
|
|
HOSPITAL ( NAME & ADDRESS ) |
|
INITIAL TREATMENT |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
NO MEDICAL TREATMENT |
|
||
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
MINOR: BY EMPLOYER |
|
||
|
T |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
MINOR CLINIC/HOSPITAL |
|
||
|
E |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
EMERGENCY CARE |
|
|
|
|
T |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
O |
WITNESSES ( NAME & PHONE # ) |
|
|
|
|
|
|
|
HOSPITALIZED > 24 HRS |
|
|||
|
|
|
|
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/ |
|
|||
|
T |
|
|
|
|
|
|
|
|
|
|
|||
|
H |
|
|
|
|
|
|
|
|
|
LOST TIME ANTICIPATED |
|
||
|
DATE ADMINISTRATOR NOTIFIED |
|
DATE PREPARED |
PREPARER'S NAME & TITLE |
|
|
|
|
|
|
||||
|
E |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
NM WCA FORM E1.2 |
EQUIVALENT TO OSHA'S FORM 301 |
FORM |
|
|||||||||||
Completion of this form is not an admission that the claim is compensable under the Workers’ Compensation Act.
|
NEW MEXICO WORKERS' COMPENSATION ADMINISTRATION |
||
Phone: (505) |
|||
FARMINGTON: |
LAS CRUCES: |
||
LAS VEGAS: |
LOVINGTON: |
||
Roswell: |
Santa Fe: |
||
FILING INSTRUCTIONS
PURPOSE: To report all alleged
completed by the employer or the employer's representative.
WHEN TO FILE: This form must be filed within 10 days of knowledge of any alleged
WHERE TO FILE: Mail the original form to the New Mexico Workers' Compensation Administration (Attention: Statistics) at the address on the front of this form. Copies must also be provided to the worker and the employer's workers' compensation insurer.
PENALTIES: Each instance of failure to file this form when required is punishable by a fine of up to $1,000.00.
INSTRUCTIONS FOR COMPLETION
FILLING IN THE SHADED AREAS IS OPTIONAL. The employer may wish, however, to use some of these areas (such as "Witnesses") for the employer's records. Expanded instructions are found in the publication Guide to Completing the Employer's First Report of Injury or Illness, available from the Administration's Albuquerque office (call either number
Please print in black ink or type, and ensure that all entries are legible before submission. An illegible or incomplete E1 may be returned.
NAIC CODE: Represents the nature of the employer's business at the location where the worker was employed at the time of injury or illness exposure; derived from the federal government publication North American Industry Classification System Manual. Include this code if known.
EMPLOYER'S LOCATION ADDRESS: Facility where the worker was employed at the time of injury, if different from mailing address.
CARRIER: Name, mailing address and telephone number of the licensed business entity issuing a contract of insurance and assuming financial responsibility on behalf of the employer. A
CLAIMS ADMINISTRATOR: Name, mailing address and telephone number of the insurance carrier, agency, third party administrator or
EMPLOYER, CARRIER OR ADMINISTRATOR FEIN: Federal Identification Number, assigned by the Internal Revenue Service.
DID SALARY CONTINUE? Shows if the employer is continuing to pay the worker's regular wages without charge to employee benefits.
DATE OF INJURY/ILLNESS: In the case of an occupational illness (arising from the worker's activity or exposure over an extended period), enter the date of diagnosis or the date first reported to the employer as possibly
DATE EMPLOYER NOTIFIED: The date the worker first notified (verbally or in writing) the employer or the employer's representative of the alleged
DATE DISABILITY BEGAN: The first full day on which the worker lost time from work due to the injury or illness.
TYPE OF INJURY OR ILLNESS: Briefly describe the nature of the injury (such as lacerations to the forearm) or illness (such as carpal tunnel syndrome). Be as specific as possible.
PART OF BODY AFFECTED: The specific part of body affected by the injury or illness (for example, right forearm, lower back).
DEPARTMENT OR LOCATION: If the accident or illness exposure did not occur on the employer's premises, enter specific address or location (for example, Client's office at 123 Main St., Yourtown, NM 87xxx). For occurrences in New Mexico, give ZIP or COUNTY.
ALL EQUIPMENT, MATERIAL OR CHEMICALS: List all equipment, materials and/or chemicals the worker was using, applying, handling or operating when the injury or illness exposure occurred. Be specific (for example, decorator's scaffolding, electric sander, paintbrush and paint). Enter "NA" if not applicable. NOTE: The items listed do not have to be directly involved in the worker's injury or illness.
SPECIFIC ACTIVITY: Describe the specific activity the worker was engaged in when the accident or illness exposure occurred (for example, sanding ceiling woodwork in preparation for painting).
WORK PROCESS: Describe the work process the worker was engaged in when the accident or exposure occurred, such as building maintenance. Enter "NA" for not applicable if not engaged in a work process (for example, if the worker was walking along a hallway).
HOW INJURY OR ILLNESS OCCURRED: Describe how the injury or illness/abnormal health condition occurred. Be very specific. Include the sequence of events and name any objects or substances that directly injured the worker or made the worker ill. (For example: worker stepped back to inspect work and slipped on some scrap metal. As worker fell, worker brushed against the hot metal.)
WORKER'S/EMPLOYER'S RIGHTS AND RESPONSIBILITIES
If you, the worker, believe that benefits are due you under the Workers' Compensation Act, and your employer or the employer's insurance carrier has failed or refused to make those benefits available to you, you have a right to file a complaint with the New Mexico Workers' Compensation Administration. Workers and employers with questions about rights or responsibilities under the Act may contact an ombudsman at any Workers' Compensation Administration regional office for information and assistance. To do so, call any of the
File Specifics
| Fact Name | Description |
|---|---|
| Governing Law | New Mexico Workers' Compensation Act |
| Filing Deadline | The form must be filed within 10 days of knowledge of the work-related injury or illness. |
| Submission Address | Workers' Compensation Administration, PO Box 27198, Albuquerque, NM 87125-7198 |
| Penalty for Non-compliance | A fine of up to $1,000.00 may be levied for each instance of failure to file the form when required. |
How to Use New Mexico Report
Filing the New Mexico Workers' Compensation Administration Employers' First Report of Injury or Illness is a mandatory process for employers to document workplace accidents or illnesses that result in more than seven days of lost work, or in the case of a worker's death. This document serves to ensure all relevant information regarding the incident is officially recorded. The completion of this form is crucial for compliance with state regulations and to facilitate any potential workers' compensation claim. The process outlined below is designed to help employers accurately complete and submit the form in a timely manner.
- Obtain the form from the New Mexico Workers' Compensation Administration website or office.
- Use black ink or type to fill out the form to ensure legibility.
- Enter the employer's name, address including ZIP code, and the location address if different, in the designated spaces at the top of the form.
- Provide the carrier/administrator claim number, OSHA log number, and report purpose code in the appropriate fields.
- Fill in the jurisdiction claim number, insured report number, and employer's location number if applicable.
- Under "Carrier," include the name, address, and phone number of the insurance carrier or administrator handling the claim.
- Check the appropriate box if the coverage is through a self-insurance arrangement.
- Provide the Federal Employer Identification Number (FEIN) for the employer, carrier, and administrator as required.
- Complete the employee information section with the employee's name, date of birth, social security number, address including ZIP code, gender, marital status, occupation/job title, NCCI class code, and employment status details.
- Record the date of injury or illness, date hired, state of hire, and if the injury or illness occurred on the employer's premises.
- Detail the type of injury or illness, part of body affected, and the department or location where the accident occurred.
- List all equipment, materials, or chemicals the employee was using when the accident or illness occurred.
- Describe the specific activity the employee was engaged in and how the injury or illness occurred, including the sequence of events and any objects or substances directly involved.
- Indicate if salary continued for the employee and if full pay was provided for the day of injury.
- Enter the physician or healthcare provider's name and address, and the hospital's name and address if applicable.
- Detail any witnesses with their names and phone numbers.
- Indicate the treatment provided initially and specify if future major medical treatment or lost time is anticipated.
- Fill in the dates when the administrator was notified, the form was prepared, and the preparer's name and title.
- Review the form for completeness and accuracy. An incomplete or illegible form may be returned, delaying the process.
- Mail the original completed form to the New Mexico Workers' Compensation Administration at the provided address. Ensure copies are also provided to the affected worker and the employer's workers' compensation insurer.
After submission, it's important to follow up with both the employee and the insurer to ensure that all necessary steps are being taken. Keep a copy of the submitted form for your records. Compliance with this procedure not only fulfills your legal obligations but also supports your employee's rights to any applicable benefits under the Workers' Compensation Act. Remember, completing this form does not constitute an admission of liability but is a required step in managing workplace injuries or illnesses.
Understanding New Mexico Report
What is the purpose of the New Mexico Workers' Compensation Administration Employers' First Report of Injury or Illness form?
This form is used to report all alleged work-related injuries or illnesses that result in more than seven days of lost work, or in the death of the worker. It serves as a mechanism for the employer, or the employer's representative, to document and notify the necessary parties about the incident. It's important to clarify that completing this form does not admit responsibility for the claim under the Workers’ Compensation Act.
When must the Employers' First Report of Injury or Illness form be filed?
Employers must file this form within 10 days of becoming aware of any alleged work-related injury or illness that leads to more than seven days of lost work. The obligation to file exists regardless of any disputes over the worker's claim of a work-related injury or illness.
Where should the form be sent?
The original form should be mailed to the New Mexico Workers' Compensation Administration, specifically to the Statistics department at the address provided on the form. Additionally, copies of the form must be provided to both the worker involved and the employer's workers' compensation insurer.
Are there any penalties for not filing the form on time?
Yes, each instance of failing to file the form as required can result in a fine of up to $1,000.00.
What sections of the form are optional to fill out?
Filling in the shaded areas of the form is optional, although some employers may choose to use these sections for their own records, such as listing witnesses. The intention behind making these sections optional is to provide flexibility for employers while ensuring essential details are reported.
How should the form be completed?
The form should be completed either by printing in black ink or by typing to ensure legibility. It's critical to make sure that all entries are clear because an illegible or incomplete form may be returned for correction.
What is the NAIC code and where should it be included?
The NAIC code represents the nature of the employer's business at the location where the worker was employed at the time of the injury or illness exposure. It is derived from the North American Industry Classification System Manual. If known, this code should be included on the form to provide clarity on the type of business where the incident occurred.
What should be done if the worker was not injured on the employer's premises?
If the accident or illness did not occur on the employer's premises, it's necessary to specify the exact address or location of where it happened, such as a client's office. For incidents occurring in New having to include to include Mexico, the ZIP or COUNTY should also be provided if possible.
Where can additional information or assistance be sought?
Employers or workers seeking more information or needing assistance with the form or the process can contact an ombudsman at any Workers' Compensation Administration regional office. A list of phone numbers is provided on the form for convenience, with services available Monday through Friday, 8 a.m. to 5 p.m.
Common mistakes
Failing to use black ink or type when filling out the form can lead to legibility issues, making it difficult for the processing team to accurately interpret the information provided.
Omitting the employer's or carrier's Federal Identification Number (FEIN) can lead to confusion and delays, as these numbers are crucial for identifying the correct entities involved in the claim.
Incorrectly or incompletely listing the type of injury or illness, as well as the part of the body affected, can result in inappropriate handling of the claim. Specific and detailed descriptions are vital for a thorough understanding and evaluation of the injury or illness.
Not specifying whether the injury or illness occurred on the employer's premises leads to a lack of context for the claim, affecting its processing and outcome.
Leaving the section about whether salary continued post-injury blank can create uncertainties in the compensation calculation, potentially affecting the benefits the worker is entitled to.
Overlooking the signature and date areas at the end of the form invalidates the submission, as these are required to verify the accuracy of the information and the identity of the preparer.
It is crucial for individuals completing the New Mexico Employers' First Report of Injury or Illness form to avoid these common mistakes to ensure the timely and accurate processing of their claims. Attention to detail and thoroughness in completion can significantly impact the outcome and efficiency of the claim's processing.
Documents used along the form
When navigating through the complexities of reporting an injury or illness under the New Mexico Workers' Compensation system, having the right documents and forms ready can streamline the process, ensuring all parties are well-informed and compliant. The New Mexico Employer's First Report of Injury or Illness form is a crucial starting point for this process. However, to fully support a workers' compensation claim, several other documents may also come into play. Understanding these documents can be incredibly helpful for employers, employees, and insurance carriers alike.
- Notice of Accident Form: To be completed by the injured employee, this form officially notifies the employer of a work-related injury or illness. It's a critical document that should be filled out and submitted to the employer as soon as possible after the incident occurs.
- Wage Verification Form: Used to verify the injured employee's wages, this document is essential for calculating compensation benefits correctly. It requires detailed information about earnings, including tips, bonuses, and any other compensation received prior to the injury or illness.
- Medical Release Form: This form authorizes the release of medical records related to the injury or illness to the employer or insurance carrier. It's an essential document for substantiating the claims made in the Workers' Compensation claim process.
- Agreement of Compensation: Once a claim is examined and accepted, this form outlines the terms of workers' compensation benefits that the injured employee will receive. Both the employer and the employee must sign this agreement, highlighting the importance of mutual understanding regarding compensation.
- Notice of Compensation Payable: Issued by the employer or insurance carrier, this document officially acknowledges that a claim has been accepted and that compensation payments will be made. It details the amount of benefits and the duration for which they will be provided.
- Final Receipt: Used to indicate the conclusion of workers' compensation benefits, this document is filed when the injured employee returns to work or has otherwise recovered from the injury or illness. It is a formal acknowledgment that compensation is no longer being paid.
Together, these documents form a comprehensive framework that supports the initial report of injury or illness. By ensuring timely and accurate completion of each form, all parties can contribute to a smoother and more effective claims process. Remember, the goal of workers' compensation is not just to provide financial assistance but also to ensure a safe and swift return to work for the injured employee. Knowledge of these documents empowers all involved parties to navigate the system with confidence and clarity.
Similar forms
The New Mexico Report form, officially known as the Employer's First Report of Injury or Illness, shares considerable similarities with various other documents used across the United States for reporting and managing workers' compensation claims. These documents serve as essential tools for employers, insurance carriers, and regulatory bodies to document and process incidents of workplace injuries or illnesses. Among these, two particular forms stand out for their relevance and comparability: the OSHA Form 301 and the IAIABC Form IA-1.
The OSHA Form 301 is one such document that bears a resemblance to the New Mexico Report form. Developed by the Occupational Safety and Health Administration (OSHA), Form 301 is an Injury and Illness Incident Report that employers must fill out to detail the specifics of an occupational injury or illness. Similar to the New Mexico Report form, it requires information about the employee, the nature of the injury or illness, how it occurred, and the outcome (such as time away from work). Both forms are designed to capture a comprehensive account of work-related injuries or illnesses, enabling employers to report these incidents accurately. They play a crucial role in maintaining workplace safety and health standards, facilitating the monitoring and prevention of future incidents.
The IAIABC Form IA-1, another document akin to the New Mexico Report form, is provided by the International Association of Industrial Accident Boards and Commissions. This form, also intended for reporting injuries or illnesses that occur in the workplace, collects similar kinds of information: details about the employee (including name, Social Security number, and job title), specifics about the injury or illness (such as date of occurrence, type, and body parts affected), and treatment information. Both the New Mexico Report form and the IAIABC Form IA-1 serve the same fundamental purpose: to ensure that workers' compensation claims are appropriately documented and processed. They support the effective management of workplace injuries and illnesses, helping to ensure that affected employees receive the benefits and care they are entitled to under respective workers' compensation laws.
Dos and Don'ts
Filling out the New Mexico Employers' First Report of Injury or Illness forms accurately is crucial for ensuring the prompt and effective handling of workers' compensation claims. Below are several important dos and don'ts to consider when completing this form:
- Do print in black ink or type the information to ensure legibility.
- Do provide detailed and specific information regarding the type of injury or illness and the part of body affected.
- Do ensure all required fields are completed to avoid delays; an incomplete form may be returned, further delaying the process.
- Do describe the sequence of events leading to the injury or illness in detail, including any objects or substances that directly contributed to the event.
- Don't leave the witness information section blank if there were any witnesses to the incident. Their accounts may be crucial to the investigation of the claim.
- Don't forget to list all equipment, materials, or chemicals the employee was using, applying, handling, or operating when the injury or illness occurred. This information is critical for understanding the circumstances of the incident.
- Don't provide vague descriptions of the injury, illness, or how it occurred. Specificity is key in understanding the nature of the incident and determining compensability.
- Don't wait longer than 10 days from gaining knowledge of the alleged work-related injury or illness that results in more than 7 days of lost work to file the form. Timely filing is crucial for compliance with state regulations.
Remember, accurately completing the New Mexico Employers' First Report of Injury or Illness form is not only a legal requirement but also a critical step in ensuring workers receive the appropriate care and compensation following workplace injuries or illnesses.
Misconceptions
When dealing with the New Mexico Workers' Compensation Administration's First Report of Injury or Illness form, there are several misconceptions that can lead to misunderstandings regarding its use and requirements. It's crucial to address these to ensure accurate and timely reporting of workplace injuries or illnesses.
- Misconception 1: Completing the form is optional.
- Misconception 2: Only injuries requiring immediate medical attention must be reported.
- Misconception 3: The form serves as an admission of liability by the employer.
- Misconception 4: The form must be completed in pen and mailed to the Workers' Compensation Administration.
- Misconception 5: All sections of the form must be filled out, regardless of relevance.
- Misconception 6: The form is only necessary for incidents that occur on the employer's premises.
To clarify:
- The form is mandatory for reporting any alleged work-related injuries or illnesses that result in more than 7 days of lost work, or in death. It's not optional and must be filed within 10 days of knowledge of such injuries or illnesses.
- Every alleged workplace injury or illness must be reported, not only those that seem severe at the onset. This includes injuries or illnesses that develop over time, such as repetitive stress injuries.
- Filing the form is a procedural requirement and does not constitute an admission of liability or agreement that the injury or illness is compensable under the Workers’ Compensation Act.
- Although the form must be completed accurately and legibly, it can be printed in black ink or typed. Moreover, submitting the form electronically may also be an option, depending on current administration processes.
- Filling in shaded areas of the form is optional and primarily for the employer's records. These sections include areas for witnesses or additional notes that may not be directly relevant to the initial report filing.
- Reportable injuries or illnesses include those that do not occur on the employer's premises if they are work-related. For instance, injuries that occur while traveling for work purposes or working remotely should also be reported.
Understanding these points is crucial for ensuring that injuries and illnesses are reported correctly and in compliance with New Mexico Workers' Compensation Administration requirements. Proper filing supports the well-being of employees and helps maintain a transparent and efficient workplace injury and illness reporting system.
Key takeaways
Here are key takeaways about filling out and using the New Mexico Workers' Compensation Administration Employers' First Report of Injury or Illness:
- The form must be used to report any alleged work-related injuries or illnesses that result in more than seven days of lost work, or in the death of a worker.
- Employers or their representatives are required to complete the form, not an admission or denial of the worker's alleged injury or illness's compensability.
- It's mandatory to file this form within 10 days of becoming aware of an alleged work-related injury or illness that results in more than seven days of lost work.
- The original form should be mailed to the New Mexico Workers' Compensation Administration, with copies provided to the worker affected and the employer's workers' compensation insurer.
- A failure to file the form as required can result in a fine of up to $1,000.00 per instance.
- For clarity and record-keeping, filling out the form in black ink or typing is recommended to ensure legibility.
- The form requires detailed information about the injury or illness, including the date of the injury/illness, type of injury or illness, part of body affected, and how the injury or illness occurred.
- Identification of all equipment, materials, or chemicals the employee was using at the time of the injury or illness is necessary unless not applicable (noted as "NA").
- Safeguards or safety equipment provided and whether they were used should be disclosed on the form.
- Information about the worker's employment status, including occupation/job title, employment status, and whether full pay was provided for the day of injury, is required.
- It's essential to include the date when the employer was notified of the injury or illness and when the disability began.
If workers believe benefits are due under the Workers' Compensation Act and those benefits have not been made available, they have the right to file a complaint with the New Mexico Workers' Compensation Administration. Employers and workers with questions about rights or responsibilities under the Act are advised to contact an ombudsman for assistance.
Other PDF Forms
Nm Board of Nursing - The inclusion of supervisor verification acts as a safeguard for the integrity of the information presented, contributing to accurate licensure records.
New Mexico Franchise Tax - Assists New Mexico in maintaining a comprehensive and compliant taxation environment for businesses.